Hiatus/Paraoesophageal Hernia Surgery
What is a Hiatus or Paraoesophageal hernia?
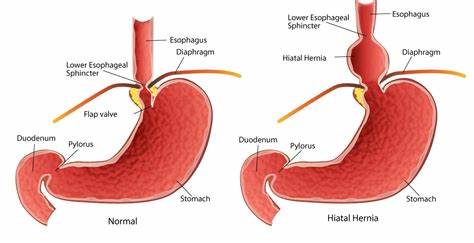
A hiatus hernia occurs when the normal opening in the diaphragm for the oesophagus becomes stretched and enlarged. This allows the upper part of the stomach to slide up into the chest.
This causes the one-way valve between the oesophagus and stomach to become faulty and commonly causes Gastric Reflux or Heartburn. Rarely large hernias can cause obstruction and pain.
Larger hiatus hernias are often referred to as Paraoesophageal hernias. Paraoesophageal hernias can involve part or in some cases the entire stomach and/or other organs to bulge up into the chest.
This causes the one-way valve between the oesophagus and stomach to become faulty and commonly causes Gastric Reflux or Heartburn.
Types of Hiatus Hernia
There are 2 main types of hiatus hernia.
- Sliding Hiatus Hernia - This is the most common type of hiatus hernia. It occurs when the junction between the oesophagus and the upper part of the stomach moves up through the oesophageal opening in the diaphragm into the chest cavity. The herniated portion of the stomach can slide back and forth, into and out of the chest.
- Rolling Hiatus Hernia - This is sometimes called a para-oesophageal hernia. In this case, part of the stomach bulges into the chest through the weakest part of the diaphragm, which is the oesophageal opening. The junction of the oesophagus and stomach stays down within the abdomen, and the top part of the stomach (the fundus) bulges up into the chest cavity. This type of a hernia normally remains in one place, sitting next to the oesophagus, and does not move in or out when you swallow.
What are the Symptoms of a Hiatus Hernia?
Most people are not troubled by their hiatus hernia, but if reflux of the acid contents of the stomach occurs (called gastro-oesophageal reflux), you may experience heartburn. This is a painful burning sensation in the chest.
Sudden regurgitation of acid fluid into the mouth can occur, especially when you lie down or bend forward. These symptoms are a problem when you go to bed and can wake you up.
Other symptoms include belching, pain on swallowing hot fluids and a feeling of food sticking in the oesophagus. Rarely excruciating abdominal pain occurs where the blood supply is cut off to that part of the stomach that has protruded into the chest. Nausea, vomiting and loss of appetite indicate an intestinal obstruction.
Suitability for Hiatus Hernia Surgery
The complicated hiatus hernia requires surgery occasionally on an emergency basis. Surgery otherwise is reserved for those patients with symptoms that cannot be controlled with medications or those patients concerned or not willing to take medication long term.
The mere presence of a hiatus hernia is not a reason for surgery. Surgical treatment is called for when a hernia results in symptoms, such as persistent heartburn or difficulty in swallowing.
Before Hiatus Hernia repair surgery
Hiatus hernia repair surgery is general safe with a low complication rate. Steps may be advised by Dr Manley for you to take prior to surgery to make it safer including;
- Advising pre operative weight loss
- Commencing a low calorie diet with a meal substitute such as optifast 2-3weeks prior to surgery. The effect of this is to decrease the bulkiness of the liver and improve the surgical view, making the operation safer
Acid inflammation and ulceration of the lower oesophagus may also require treatment.
Laparoscopic Hiatus Hernia Repair
Hiatus hernias and paraoesophageal hernia repairs are typically performed via a laparoscopic technique.
Laparoscopic or keyhole surgery has many benefits compared to traditional methods of anti-reflux surgery involving large incisions. Benefits include shorter hospital stay, reduced risk of organ injury, wound infection and reduced post-operative pain.
Rarely in the cases of redo/revisional surgery or with extremely large hernias alternative approaches may need to be considered including operating via the thoracic cavity.
Hiatus hernia repair aims to return the stomach and/or other contents of the hernia back to their normal position within the abdominal cavity without tension and reinforce the weakened area through which the hernia has protruded.
Hiatus hernia repair is often performed in conjunction with a fundoplication.
Read more about Fundoplication/Anti-reflux Surgery
Hiatus hernia repair is performed under general anaesthesia and most patients stay 1-2 nights in the hospital.
Steps involved in the procedure include:
- Your surgeon makes five small incisions in the upper abdomen and inserts a telescope and a number of other instruments into the abdomen. The procedure is done by watching a monitor.
- The liver is gently retracted to allow the surgeon to view the hernia
- The stomach and hernia contents are dissected free from any attachments within the thoracic cavity so it is returned to the normal anatomical location without tension
- The gap in the diaphragm through which the oesophagus normally passes through to enter the abdominal cavity has typically enlarged to allow the stomach to migrate into the chest. This gap returned to normal dimensions with sutures and occasionally absorbable mesh
- A tube in placed in the oesophagus to ensure the repair is not “too tight”
- The surgeon then usually wraps the upper part of the stomach, (called the fundus), around the lower oesophagus to create a valve, suturing it in place. (fundoplication)
- The laparoscope and other instruments are removed and the gas released.
- Local anaesthetic blocks are used to reduce post-operative discomfort
- The tiny incisions are then closed.
Risks of laparoscopic Hiatus Hernia Repair
There are some risks of laparoscopic hernia repair that are shared by all operations, these risks occur rarely. They include heart attack, stroke, a clot in the lungs (pulmonary embolus), significant bleeding, infection and injury to the bowel.
There are some risks that are specific to laparoscopic hiatus hernia repair:
- Injury to other organs and structures including the spleen
- Occasionally patients have difficulty swallowing after the operation. If this occurs it usually improves with time
- Bloating and discomfort from gas build up may occur because the person is not able to burp.
- Excess gas.
- Recurrent hernia/reflux in the future
Discharge From Hospital
You will be able to go home within couple of days after the operation once you are comfortable and able to take a puree diet.
Recovery After The Procedure
After the surgery,
Wound Care
- Care should be taken with your wound.
- Waterproof dressings are applied so you can shower
- They should be removed after 5 days.
Pain Management
- You may feel soreness around the incision areas.
- Your surgeon may give you prescription pain medicine or recommend non-steroidal anti-inflammatory drugs (NSAIDs) for the first few days to keep you comfortable.
- You may experience discomfort in the abdomen, chest, or shoulder area for a couple of days either due to the gas from surgery or internal sutures.
Diet
- Your surgeon will instruct you about your diet and activity restrictions. Dietary restrictions are progressively lifted and usually unrestricted within 6 weeks following the surgery
Activity
- Shortly after surgery, you can gradually resume your daily activities,
- You are encouraged to start walking as early as possible to reduce the risks of blood clots and pneumonia, and
- You are advised not to lift heavy objects for 4-6 weeks.
Work
- You will be able to get back to work usually within 2 weeks.
Contact your doctor immediately if you have a fever, chills, increased pain, bleeding or fluid leakage from the incisions, chest pain, shortness of breath, leg pain or dizziness.